

 FP0654 : Sewing Needle Micro Capsulotomy : New technique to prevent Argentinian flag sign
FP0654 : Sewing Needle Micro Capsulotomy : New technique to prevent Argentinian flag signDr.Rajendra Prasad
Dr.ANURAG BADHANI
Semi Finals
Abstract
We describe an efficient new technique, “Sewing Needle Micro Capsulotomy,” to prevent Argentinian flag sign during capsulorrhexis in patients with intumescent pearly white mature cataracts. Sewing needle micro capsulotomy utilizes the principle of ballpoint sewing machine needle system to puncture the stretched tight anterior capsule. Round pointed tip of the sewing needle micro capsulotome when pierce tight and stretched anterior capsule create a hole, which is similar to mini capsulorhexis with round continuous circular edge, without any discontinuity. Round hole micro capsulotomy do not tear away with the sudden out burst of intralenticular fluid and disruptive lateral separation force generated by the stretched tight anterior capsule. Evacuation of liquefied cortical material through the hole decompresses the capsular bag and allows for intralenticular pressures to equilibrate prior to the initiation of capsulorrhexis thus prevent radial extension of capsular tear.
Full Text
ABSTRACT
The Argentinian flag sign is a known complication in intumescent white cataracts, which arises instantly after an initial prick with a sharp hypodermic needle on a stretched out anterior capsule. Increased intralenticular pressure is believed to be responsible for propagation of the initial prick into a radial capsular tear. However, it is the ‘linear cut’ configuration of the initial prick, created by the hypodermic needle on the tense anterior capsule, which spontaneously opens up and propagates towards the periphery along its margins. To overcome this we devised a novel instrument sewing needle microcapsulotome to puncture the capsule and create a single or multiple round openings with smooth margins allowing the bag to decompress satisfactorily without yielding to disruptive intralenticular forces. This technique of sewing needle microcapsulotomy, to prevent Argentinian flag sign, was found to be highly effective and safe in a series of surgeries on intumescent cataracts.
INTRODUCTION
Intumescent white cataracts pose various challenges for the operating surgeon. These forms of cataracts have liquefied, hyper-hydrated and swollen lenticular material, with increased intralenticular pressure and a relatively tense stretched out anterior lens capsule. Once the surgeon attempts to begin the capsulorhexis, a spontaneous radial extension of the capsular tear towards the periphery may occur. The Argentinian Flag Sign, a well known complication during capsulorhexis in intumescent white cataracts, is the appearance of the stained blue anterior capsule on either sides of the white cataract, mimicking the pattern of Argentina’s flag, and was described by Daniel Mario Perrone, MD. [1]
In some cases this radial extension of the tear may occur later during the course of continuous curvilinear capsulorhexis due to various other factors. These include insufficient chamber maintenance with viscoelastic devices or excess posterior pressure such as exhibited during patient exertion or valsalva. [2] The loss of rhexis margin may even extend to the posterior capsule leading to vitreous loss, loss of lens material to the posterior segment, poor capsular support for intraocular lens implantation as well as corneal endothelial damage from extensive intraocular manipulation and extended surgical time. [3,4,5,6] This adversely affects the anatomical and functional results of surgery.
It is therefore prudent to prevent Argentinian flag sign formation in intumescent white cataracts. Several methods have been described such as Femtosecond laser assisted capsulotomy, Nano-pulse capsulotomy (Zepto, Mynosys Cellular Devices, Inc.) and Capsulaser (Excel-Lens, Inc.), which employs selective absorption of the laser by the trypan blue stained capsule to create a capsulorhexis. Although these technologies automate the capsulotomy and reduce the dependence on surgical skill, they also add significantly to the cost of the cataract procedure.[7] Phaco-capsulotomy is another technique where simultaneous puncture of the anterior capsule and decompression of the capsular bag is done with the help of phaco-probe [8] Potential complications of phaco-capsulotomy include wound burn and zonular dehiscence due to excessive manipulation. The configuration of capsular opening created is almost unpredictable and also has irregular margins, which may later aid in propagating a radial extension. [9] Furthermore, the safety and efficiency of these techniques to automate a complete capsulorhexis in intumescent cataracts have not been established yet.
Manual capsulorhexis techniques like two staged capsulorhexis or a mini-capsulorhexis have been described in intumescent cataracts to avoid Argentinian flag sign. [10,11] Small needle aspiration technique is one such manual capsulorhexis technique, which has been used widely by many surgeons. [12,13] This involves pricking the anterior capsule with a sharp 26 G or 30 G hypodermic needle followed by simultaneous aspiration of liquified lens matter to decompress the bag. A modified version of the same has been described wherein the capsular prick and aspiration is performed before creating the corneal incisions. In spite of using these techniques, peripheral extension of the capsular tear has still been frequently seen, during the hypodermic needle prick of the tense anterior capsule, even before initiating the aspiration of liquid cortex.
Despite many techniques the problem of radial extension of the capsular tear continues to be a challenge in intumescent white cataract surgery. Several mechanisms have been described earlier for the propagation of radial tear in these intumescent white cataracts. The concept of anterior and posterior pressurised intralenticular compartment system was put forth by, Figueiredo et al. They postulated that it is the posterior intralenticular pressure between the nucleus and posterior capsule of the lens, rather than the vitreous pressure, which pushes the nucleus forward and can lead to capsulorhexis extension even after the use of preoperative mannitol or aspiration of intralenticular fluid from the anterior compartment. [14]
There had to be other factors responsible, which assist the raised intralenticular pressure to propagate the splitting of capsule after the initial prick, as it was noticed that the capsule usually splits open even before, or at times during the aspiration of liquified lens matter with sharp needle. We referred back to a series of surgical videos of intumescent white cataracts where Argentinian flag sign was noted. On close examination we noticed that the sharp beveled hypodermic needle (26 G, 30 G) being used to open up the anterior capsule to initiate rhexis and decompress the intralenticular pressure, always created a ‘linear cut’ along the plane of needle bevel. We also observed that the linear cut configuration of the initial prick on a capsule under tension always extended radially and spontaneously along the open margins of the cut but never perpendicular to the linear cut. This configuration of the opening made on the capsule by the prick with a sharp hypodermic needle is what grabbed our attention.
In reality it is not only the raised intralenticular pressure which causes the extension of tear but it is the ‘linear cut’ configuration of the tear on the anterior capsule created by the sharp edge of the beveled hypodermic needle cystotome or sharp tipped rhexis forceps, responsible for the split in the anterior capsule. Raised intralenticular pressure with sudden forward thrust of the nucleus against the back of the anterior capsule triggers a disruptive force which thereafter splits the initial linear cut into a complete anterior capsular tear, spontaneously extending towards the periphery. This observation also adds to the known mechanism of occurrence of Argentinian flag sign in intumescent white cataracts. [Figure 1]
Henceforth we came up with a hypothesis that if we were able to manually create an opening in the anterior capsule which had a round regular configuration, like a capsulotomy in true sense instead of a linear cut, we may provide resistance against the forward thrust of intralenticular pressure, thus preventing Argentinian flag sign. We incorporated the sewing needle tip to design to develop a novel instrument that would puncture the anterior capsule creating an opening which had a smooth round configuration, allowing liquified lens matter to egress and decompress the bag without propagating a radial extension of tear.
After a few rounds of modifications we came up with a unique but simple device, sewing needle microcapsulotome, a hook with a round knurled handle, angled 60 degree to the distal shaft which ends in a sharp pointed round tip approximately 0.75 mm in length, 0.60 mm in diameter, angled at 90 degree. [Figure 2, 3]
SURGICAL TECHNIQUE
After routine incisions, the anterior capsule is stained with 0.06% trypan blue dye to enhance the visibility [9]. In accordance with soft shell technique, dispersive ophthalmic viscosurgical device (OVD) (Viscoat, DisCoVisc) is injected into the anterior part of the anterior chamber followed by flattening of the anterior lens capsule with the injection of highly cohesivee OVD like sodium hyaluronate (1.4% Healon GV, 2.3% Healon 5).
Using the main corneal incision, sewing needle microcapsulotome is inserted into the anterior chamber and the tip of the needle is placed vertically at 90 degrees over the centre of the anterior capsule. Under direct visualisation, tip is then moved downwards to penetrate through the taut anterior capsule. Sewing needle microcapsulotome puncture creates a round opening with smooth margins at the centre of the anterior capsule. Once the process of microcapsulotomy is complete, the tip of microcapsulotome is removed vertically without making any sideways or horizontal movements [Figure 4,5].
On pricking the taut anterior capsule, pressurised intralenticular fluid spontaneously egresses out through the microcapsulotomy. Since the pointed round tip of microcapsulotome creates a round continuous hole, it provides resistance to the force of sudden outburst of intralenticular pressure, helping prevent the pre-evacuation splitting of anterior capsule.
As soon as the micro capsulotomy is successfully performed, complete decompression of the intralenticular compartment is further done by evacuation of the fluid with delicate shove, twist, and wobble manipulations of the nucleus with the visco cannula. Decompression of the posterior intralenticular compartment can be achieved by tipping the edge of the nucleus at equator posteriorly with the cannula tip so that the fluid trapped between nucleus and posterior capsule flows out anteriorly. More than one microcapsulotomies, around the central opening, can be created to release multiple pockets of fluid in the capsular bag. [Figure 5]
Once the decompression is complete, anterior chamber is reformed with cohesive viscoelastic to compensate for the loss of intralenticular volume and to pressurise the anterior chamber so that anterior capsule is flattened prior to initiation of the capsulorhexis. An intended 5.0–5.5 mm capsulorrhexis is initiated after tearing the central hole using a rhexis forceps and easily completed without the risk of peripheral extension of the rhexis.
Since nucleus in intumescent cataract is free within the liquefied cortico-epinuclear complex hydrodissection is generally not required. Nuclear segmentation is done with any suitable chopping technique and phacoemulsification is performed with standard parameters followed by intraocular lens implantation in the capsular bag.
We compared the efficacy of sewing needle microcapsulotomy in preventing Argentinian flag sign with the known small needle aspiration technique in 20 cases of intumescent white cataracts (n=10 in each group). Cases were randomly allotted to each group and were single blinded. All surgeries were, performed by a single surgeon in a single surgical setup. We found that none of the cases developed Argentinian flag sign where we used the sewing needle microcapsuolotome to puncture the taut anterior capsule. A smooth round microcapsulotomy was created in a single attempt in all cases and bag was sufficiently decompressed. In none of the cases was the capsulorhexis margin lost during the completion of rhexis later. While using the small needle aspiration technique, in 6 cases the Argentinian flag sign was noted as soon as the sharp hypodermic needle was used to prick the anterior capsule, even before aspiration of lens fluid was attempted. In 2 cases out of the 4 where aspiration was possible, partial splitting and widening of anterior capsular opening was noted which was later converted into a round capsulorhexis with significant manipulation and loss of surgical time. The statistical analysis suggested that sewing needle microcapsulotomy is a safe, simple and effective technique to avoid Argentinian flag sign in intumescent white cataracts (p=0.011).
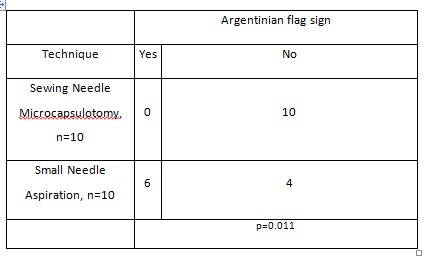
Table 1:
DISCUSSION
The Argentinian flag sign can complicate a surgery for intumescent white cataract during early surgical steps. The widely accepted recommendation to prevent Argentinian flag sign till date involves attempting to decompress the capsular bag by pricking it with a 26 G or 30 G sharp hypodermic needle followed by aspiration of liquified lens matter. This was based on the known fact that raised intralenticular pressure leading to forward nuclear thrust is solely responsible for splitting of the capsule.
We have demonstrated here that it is the sharp tip hypodermic needle, routinely used to puncture the capsule, which has been triggering the mechanism for Argentinian flag sign even before the raised intralenticular pressure comes into play. The linear cut produced by the sharp tip hypodermic needle on a stretched out anterior capsule always has a tendency to open up and extend towards the periphery along its open margins, forming the Argentinian flag sign.
An ideal instrument to open up the tense capsule in intumescent cataracts would be the one which creates a round opening with smooth margins, in real sense a capsulotomy, so that the margins hold resistance against the ensuing forward thrust, hence preventing capsular splitting. The simple yet highly effective tool, sewing needle microcapsulotome has been designed to create a single or multiple microcapsulotomies on the anterior capsule to decompress the bag. Additional manoeuvres like milking out the liquified lens matter through the microcapsulotomies using a visco-cannula can be performed for further decompression. Thereafter the capsulorhexis can be completed as done routinely.
The sewing needle microcapsulotomy technique, along with a new understanding of the factors responsible for Argentinian flag sign, will help the surgeons tackle intumescent white cataract surgeries with confidence.
WHAT WAS KNOWN:
- In intumescent white cataracts spontaneous peripheral extension of the initial tear created on anterior capsule by sharp tip hypodermic needle leads to Argentinian flag sign.
- Till date it was known that the raised intralenticular pressure leading to forward thrust of the nucleus is solely responsible for the extension of the tear to periphery, to counter which small needle aspiration techniques had been described.
- In spite of using needle aspiration techniques, the Argentinian flag sign is known to occur while pricking the capsule, even before attempting to aspirate liquified lens material, thus suggesting a role of factors other than just raised intralenticular pressure.
WHAT THIS PAPER ADDS:
- In intumescent white cataracts, it is primarily the ‘linear cut’ configuration of the initial prick made by sharp hypodermic needle on the anterior capsule, which has the potential to spontaneously extend along its open edges aided by raised intralenticular pressure, leading to Argentinian flag sign.
- The technique of sewing needle microcapsulotomy creates an opening in the anterior capsule which has a round regular configuration, like a capsulotomy in true sense, that provides resistance against the disruptive force triggered by the high intralenticular pressure, thus preventing Argentinian flag sign.
- This simple yet highly effective novel tool- sewing needle microcapsulotome creates single or multiple microcapsulotomies to adequately decompress the bag prior to the initiation of capsulorhexis.
REFERENCES
- Perrone DM. Argentinean flag sign is the most common complication for intumescent cataracts. Ocul Surg News. 2000 Dec 15; US Edition.
- Vajpayee RB, Bansal A, Sharma N, Dada T, Dada VK. Phacoemulsification of white hypermature cataract. J Cataract Refract Surg 1999; 25:1157–1160.
- Ermis, SS, Ozturk F, Inan UU. Comparing the efficacy and safety of phacoemulsification in white mature and other types of senile cataracts. Br J Ophthalmol 2003; 87:1356–1359.
- Carifi G, Miller MH, Pitsas C, Deshmukh RR, Maurino V. Complications and outcomes of phacoemulsification cataract surgery complicated by anterior capsule tear. Am J Ophthalmol 2015; 159:463-469.
- Rao SK, Padmanabhan P. Capsulorhexis in eyes with phacomorphic glaucoma. J Cataract Refract Surg 1998; 24:882–884.
- Little BC, Smith JH, Packer M. Little capsulorhexis tear-out rescue. J Cataract Refract Surg 2006; 32:1420-1422.
- Titiyal JS, Kaur M, Singh A, Arora T, Sharma N. Comparative evaluation of femtosecond laser-assisted cataract surgery and conventional phacoemulsification in white cataract. Clin Ophthalmol 2016; 10:1357–1364.
- Teng CC. Preventing the Argentinian Flag Sign: Phaco capsulotomy. Eye World. Accessed September 15, 2020. https://www.eyeworld.org/article-preventing-the-argentinian-flag-sign–phaco-capsulotomy
- Gimbel HV, Neuhann T. Development, advantages, and methods of the continuous circular capsulorhexis technique. J Cataract Refract Surg 1990; 16:31–37.
- Gimbel HV. Two-stage capsulorhexis for endocapsular phacoemulsification. J Cataract Refract Surg 1990; 16:246–249.
- Kara-Junior N, Santhiago MR, Kawakami A, Carricondo P, Hida WT. Mini-rhexis for white intumescent cataracts. Clinics (Sao Paulo) 2009; 64:309-312.
- Perrone DM, Perrone LD, Blanco A. Techniques to avoid Argentina flag sign. American Academy of Ophthalmology. Accessed September 15, 2020. https://www.aao.org/clinical-video/techniques-to-avoid-argentinian-flag-sign.
- Dhingra D, Balyan M, Malhotra C, Rohilla V, Jakhar V, Jain AK. A multipronged approach to prevent Argentinian flag sign in intumescent cataracts. Indian J Ophthal 2018; 66:9:1304-1306.
- Figueiredo CG, Figueiredo J, Figueiredo GB. Brazilian technique for prevention of the Argentinean flag sign in white cataract. J Cataract Refract Surg 2012; 38:1531-1536.
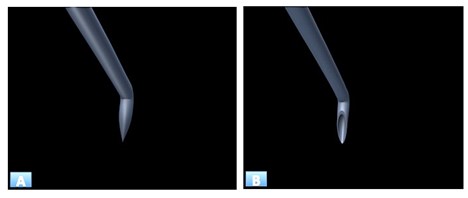
FIGURE LEGENDS
Figure 1: (A) Rajendra Prasad’s sewing needle microcapsulotome : Round pointed tip create round hole micro capsulotomy similar to mini capsulorhexis with round continuous circular edges without any discontinuity. (B) Ultra sharp beveled stain less steel hypodermic needle: Sharp tip functions like a knife and create a discontinuous slit when puncture the capsule.
Leave a Comment