
 FP0083 : Opportunistic screening of ametropia and amblyogenic factors in children using Brückner test.
FP0083 : Opportunistic screening of ametropia and amblyogenic factors in children using Brückner test.Dr. MIHIR TRILOK KOTHARI
Dr.GOURAVI UPADHYE
Abstract
Aim: To assess validity of the red reflex testing by a pediatrician for the screening of children in a pediatric OPD. Methods: In this prospective operational research, 120 consecutive children aged 1-16 years were screened by a pediatrician, pediatric ophthalmologist (PO), plus optix S12 vision screener and a pediatric optometrist (gold standard). Results: Mean age of the children was 5.2 years, 50% were boys. Out of 35 children who failed, pediatrician could identify 31, PO 29 and S12 screener 30; giving rise to a high sensitivity 88.6% and negative predictive value of 92.2% for the test in the hands of pediatrician. The lowest specificity (55%) for the test was also in the hands of Pediatrician. The accuracy was highest with S12 vision screener (85%) followed by PO (70%) and the pediatrician (65%). Conclusion: The Brückner test is a low cost, rapid screening test to rule out ametropia and amblyogenic factors in the hands of a pediatrician in a busy pediatric opd.
Full Text
The American Academy of Pediatrics currently recommends red reflex assessment as a component of the eye evaluation in the neonatal period and during all subsequent routine health supervision visits. The red reflex test also called Brückner test aims to identify opacities in the visual axis and pathologies of the posterior segment. It diagnoses the common causes of childhood blindness that includes congenital cataract, undiagnosed amblyopia, retinoblastoma and corneal opacities. However Brückner test can also be used to assess other amblyogenic factors namely ametropia, anisometropia and squint, especially in preverbal children. In the hospital based settings the sensitivity of the Brückner test was 87.5% and specificity 84.1%; the positive (PPV) and negative predictive (NPV) value was 71.8% and 93.6% making the test a useful, ultralow cost, rapid screening tests in the hands of the Optometrist and the Pediatric Ophthalmologist. In a population based screening program, the test was found useful for the screening in the hands of the Pediatrician.
Since red reflex test is anyways mandated as per the preferred practice guidelines for the Pediatricians as a routine screening test for preverbal children, we decided to evaluate the reliability of Brückner test in the hands of a Pediatric resident in a routine hospital based Pediatric OPD (outpatient department).
Subjects and methods:
The study was carried out in the outpatient Pediatric department of Jupiter hospital, Thane
After obtaining permission from the institutional ethics committee. Ten percent of all eligible children presenting in the pediatric outpatient department of Jupiter Hospital between 1- 16 years of age, of both sexes and whose parents had signed written informed consent were included. Children with the history of ocular surgery, nystagmus, clinically visible strabismus, congenital anatomical abnormalities of eye, poor general condition and uncooperative patients were excluded.
The data was entered in the MS-Excel-2010 and analysed using SPSS-16 software. The test was evaluated using 2×2 Bayesian Table and the interrater reliability was analysed using the Kappa statistic. The P value less than 0.05 was taken as statistically significant.
To check the validity, various parameters like sensitivity, specificity, positive predictive value & negative predictive value & accuracy were calculated.
- The Pediatric resident was trained to detect red reflex abnormalities in children by teaching optics of red reflex testing using didactic lecture and simulation on a dummy eye. The resident was asked to perform the technique (monocular, binocular and dynamic) on patients alongside with a trained Pediatric Ophthalmology fellow.
- Initially the red reflex test was performed by the trained Pediatric resident on children fulfilling the inclusion and exclusion criteria in the Pediatric Outpatient Department using an ophthalmoscope (Heine Germany Beta 200) at a distance of one meter.
- Both eyes were illuminated simultaneously by ophthalmoscope with the child looking at a distant object six meters away and the lens dial was adjusted till the pupillary red reflex was focused.
- Presence of any media opacities, difference in colour of red reflex, anisocoria, leukocoria was noted.
- Presence of amblyogenic factors like squint, anisometropia were noted.
- The position and size of pupillary crescent was noted and labelled as: emmetropia (normal crescent), hypermetropia (hypermetropic crescent), myopia (myopic crescent) to detect abnormalities of refraction.
- Presence or absence of astigmatism was noted based on the position of the pupillary crescent.
- Dynamic Distant Direct Ophthalmoscopy for testing accommodation was done and any accommodation failure was ruled out.
- Any other eye abnormalities during red reflex testing was noted.
- Results of red reflex testing was labelled as pass if normal and fail if any abnormality was noted in the red reflex testing of either eye each by the Pediatric resident and Pediatric Ophthalmology fellow.
- Retinoscopic measurements obtained using an automated Photoscreener in a dark room was noted for both eyes and was labelled as pass if normal and fail if abnormal (according to the American Academy of Pediatrics – Preferred practice guidelines for correction of refractive errors in children and GPOS criteria )
- Cycloplegic refraction was done 30 minutes after instilling short acting cycloplegic and compared with the findings of the Optometrist (post cycloplegic refraction/ retinoscopic findings).
- Post cycloplegic retinoscopic measurements of the Optometrist was noted for both eyes and was labelled as Pass if normal ,Fail if abnormal (according to the American Academy of Pediatrics Preferred practice guidelines for correction of refractive errors in children and GPOS criteria )
Table 1. Cut off values for crescent measurement and cycloplegic refraction 2
| Refractive error | Pattern of crescent | Size of crescent | True positive |
| Myopia | Inferior crescent | >1 mm | >/= -1 D |
| Astigmatism | crescent anywhere | >1 clock hour decentered | >/= 1.5 D |
| Hypermetropia | Superior crescent | >/= 2 mm | >/= 1D |
| Emmetropia | Superior crescent | < 2 mm | < 1D |
Table 2: criteria for refractive error correction in children
| AGE | Age 1 to <2 years* | Age 2 to < 3 years* | Age 3 to <4 years* | Age 4 years and more# |
| Isometropia | ||||
| Myopia | 4.00 D or more | 3.00 D or more | 2.50 D or more | 1.00 D or more |
| Hypermetropia | 5.00 D or more | 4.50 D or more | 3.50 D or more | 3.00 D or more |
| Hypermetropia with esotropia | 2.00 D or more | 1.50 D or more | 1.50 D or more | 1.5 D or more |
| Astigmatism | 2.50 D or more | 2.00 D or more | 1.50 D or more | 1.5 D or more |
| Anisometropia | ||||
| Myopia | 3.00 D or more | 3.00 D or more | 2.50 D or more | 1.5 D or more |
| Hyperopia | 2.00 D or more | 1.50 D or more | 1.50 D or more | 1.5 D or more |
| Astigmatism | 2.00 D or more | 2.00 D or more | 1.50 D or more | 1.5 D or more |
*American Academy of Pediatrics Preferred Practice Pattern guidelines criteria for refractive errors in Children
#GPOS (Group of Pediatric Ophthalmologists and Strabismologists ), Mumbai criteria
The result of Kappa were interpreted as follows
<0.2 – Negligible agreement
0.2-0.4 – Minimal agreement
0.4-0.6 – Fair agreement
0.6-0.8 – Good agreement
>0.8 – Excellent agreement
Results:
Total 120 children were examined by all 4 observers. The mean age was 5.2 yrs (1-15 yrs.).
Table 3: Gender Distribution of the Participants of study
| SEX | Frequency | Percent |
| Female | 61 | 50.8 |
| Male | 59 | 49.2 |
| Total | 120 | 100.0 |
Image 1: gender distribution of the study participants
Table 4: screening results by observers
| Pediatrician | Ophthalmologist | Photo screener | Optometrist | |
| Pass | 51 (42.5%) | 61 (50.0%) | 77 (64.2%) | 85 (70.8%) |
| Fail | 69 (57.5%) | 59 (49.2%) | 43 (35.8%) | 35 (29.2%) |
| Total | 120 | 120 | 120 | 120 |
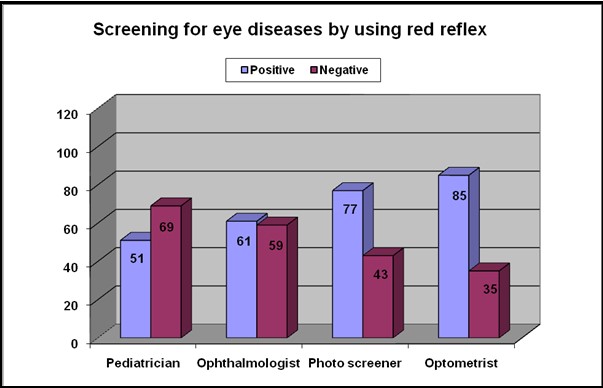
Image 2: Screening results by the participants
Table 5: Comparison between Pediatric Resident and Optometrist (Gold standard–post cycloplegic retinoscopy) findings
| Optometrist | Total | |||
| Fail | Pass | |||
| Pediatric Resident | Fail | 31 | 38 | 69 |
| 88.6% | 44.7% | 57.5% | ||
| Pass | 4 | 47 | 51 | |
| 11.4% | 55.3% | 42.5% | ||
| Total | 35 | 85 | 120 | |
| 100.0% | 100.0% | 100.0% | ||
Κ = 0.341 (Minimal agreement) P < 0.001 (Significant) (Cohen’s kappa coefficient)
Table 6: Comparison between findings of Ophthalmologist and Optometrist (Gold standard – post cycloplegic retinoscopy )
| Optometrist | Total | |||
| Fail | Pass | |||
| Ophthalmologist | Fail | 29 | 30 | 59 |
| 82.9% | 35.3% | 49.2% | ||
| Pass | 6 | 55 | 61 | |
| 17.1% | 64.7% | 50.8% | ||
| Total | 35 | 85 | 120 | |
| 100.0% | 100.0% | 100.0% | ||
Κ = 0.396 (Minimal agreement) P < 0.001 (Significant) (Cohen’s kappa coefficient)
When both the decisions were compared, it was shown that overall agreement was 70 % with simple kappa value 0.396 (Minimal agreement) which was statistically significant (p<0.001).
Table 7: comparison between findings of photoscreener and optometrist (gold standard-post cycloplegic retinoscopy)
|
|
Optometrist | Total | ||
| Fail | Pass | |||
| Photo screener | Fail | 30 | 13 | 43 |
| 85.7% | 15.3% | 35.8% | ||
| Pass | 5 | 72 | 77 | |
| 14.3% | 84.7% | 64.2% | ||
| Total | 35 | 85 | 120 | |
| 100.0% | 100.0% | 100.0% | ||
Κ = 0.660 (Good agreement) P < 0.001 (Significant) (Cohen’s kappa coefficient)
When both the decisions were compared, it was shown that overall agreement was 85 % with simple kappa value 0.660 (Good agreement) which was statistically significant (p < 0.001).
Table 8: comparison between findings of Pediatric resident and Ophthalmologist .
| Ophthalmologist | Total | |||
| Fail | Pass | |||
| Pediatric Resident | Fail | 54 | 15 | 69 |
| 91.5% | 24.6% | 57.5% | ||
| Pass | 5 | 46 | 51 | |
| 8.5% | 75.4% | 42.5% | ||
| Total | 59 | 61 | 120 | |
| 100.0% | 100.0% | 100.0% | ||
Κ = 0.667 (Good agreement) P < 0.001 (Significant) (Cohen’s kappa coefficient)
When both the decisions were compared, it was shown that overall agreement was 83 % with simple kappa value 0.667 (Good agreement) which was statistically significant (P < 0.001).
Table 9: Comparison of screening results of Pediatrician, Ophthalmologist & Photo screener with Optometrist
| Pediatrician | Ophthalmologist | Photo screener | |
| Sensitivity | 88.6 | 82.9 | 85.7 |
| Specificity | 55.3 | 64.7 | 84.7 |
| PPV | 44.9 | 49.2 | 69.8 |
| NPV | 92.2 | 90.2 | 93.5 |
| Accuracy | 65.0 | 70.0 | 85.0 |
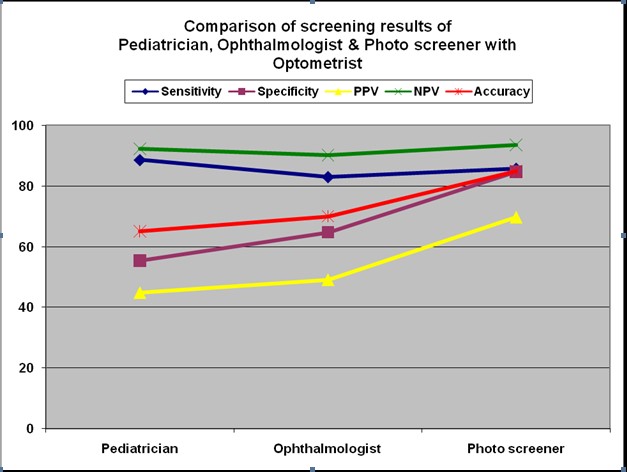
Image 3: Comparison of screening results of Pediatrician,Ophthalmologist and Photoscreener with Optometrist
Discussion
Red reflex examination in routine Pediatric practice is a very simple, low cost and effective way to screen children for eye diseases. Our study aimed at assessing the validity and precision of red reflex testing performed by a trained Pediatric resident to screen eye diseases in children aged between 1-16 years presenting to Pediatric outpatient department. We studied 120 children who came to the Pediatric outpatient department from 1/3/2019 to 30/4/2019. All 120 children were examined by all 4 observers. The mean age was 5.2 yrs. In our study, majority were females 61(50.2%) and 59 (49.8%) were male. Red reflex test could be completed for all recruited subjects. The time taken to complete this test was approximately 2 minutes per subject.
The Pediatrician identified 69 subjects had failed the red reflex testing and 51 had passed the red reflex test [ Table 8 ] as compared to the Ophthalmologist findings in which 59 subjects had failed and 61 subjects had passed the red reflex test. When both the decisions were compared it was shown that overall agreement was 83% with simple kappa value 0.667 (good agreement) which was statistically significant (p <0.001) [Table 8].
The red reflex test done by a trained Pediatric resident had a sensitivity of 88.57% (95 % confidence interval – 73.2% , 96.80 % ) and specificity of 55.29 % (95 % confidence interval – 44.11 % , 66.09 %) as compared to the red reflex testing done by trained Pediatric Ophthalmology fellow with sensitivity of 82.9 % (95 % confidence interval-66.35% , 93.44 % ) and specificity of 64.71 % (95 % confidence interval -53.59 % , 74.77 %) when the results of both observers were compared with the post cycloplegic retinoscopy findings of the Optometrist (gold standard) [Table 5 and Table 6 ].The red reflex test in the hands of the trained Pediatric resident and that of trained Ophthalmology fellow had high negative predictive value of 92.2 % and 90.2 % respectively. We could conclude that red reflex test done by a Pediatric resident is fairly sensitive and has high negative predictive value making it a good screening test to detect eye diseases in routine Pediatric practice by a Pediatrician.
Mihir T Kothari et al studied the use of Brückner test as a rapid screening test to detect significant refractive errors in children. Ninety-six subjects were examined. The Ophthalmologist identified 131 eyes as ametropic and 61 eyes as emmetropic. The Brückner test had sensitivity 91%, specificity 72.8%, positive predictive value 85.5% and negative predictive value 83.6% which was similar to the results of our study.
.Jalis M et al also used the Brückner test for the detection of significant refractive errors in children. Brückner test was performed in children upto 15 years of age with a direct Ophthalmoscope and the position and size of pupillary crescent was noted. Subsequently, noncycloplegic and cycloplegic auto-refraction was performed using auto-refractometer. The results were published in the Journal of Rawalpindi Medical College. 2015 Dec 30;19(3):200-3 .
Saiju R et al in their study measured the effectiveness of the Brückner red reflex test for screening of posterior segment opacities in children. Patients with abnormal Brückner tests had their eyes dilated for further investigations. 172 patients (97 boys and 75 girls ) were included in the study. Twenty-three had abnormal Brückner test results in either one or both eyes. The specificity of this test was 98.7%. The screening test had a positive predictive value of 90.5% and a negative predictive value of 97.4%. The study concluded that Brückner test screening is a sensitive and specific marker for detecting the posterior segment opacities in children, and recommended utilizing the test to evaluate these problems where other technologies are rare. The results were published in the Kathmandu University Medical Journal. 2012;10 (2):23-6.
In our study of 120 patients ,the retinoscopy findings of the photoscreener when compared with that of the optometrist (gold standard) showed a sensitivity of 85.7% (95 % confidence interval -69.74 % , 95.19 %) specificity of 84.71 % (95 % confidence interval- 75.27 % , 91.60 %) and a negative predictive value of 93.51 % .[Table7 ].This showed that the photoscreener is superior in detecting refractive errors & astigmatism in children as compared to manually performed red reflex testing done by the trained Pediatric resident
Paysse EA et al studied the ability of Pediatric residents to differentiate an asymmetric from a symmetric red reflex in patients with anisometropia and microstrabismus using the Brückner reflex and the Medical Technology Innovations (MTI) photoscreener. A prospective, masked, case-control study was performed by twelve Pediatric residents who evaluated 10 study patients and 6 control subjects in a masked manner in 2 separate sessions, using the Brückner reflex or the MTI photoscreener, evaluating for asymmetric (abnormal) or symmetric (normal) red reflexes between the 2 eyes. The pediatric residents had a mean correct score of 82% (69%–100%) using the MTI photoscreener versus a mean correct score of 65% (44%–81%) using the Brückner reflex (McNemar test: < 0.01). The sensitivity of the MTI photoscreener evaluation was 89% in comparison to 61% for the Brückner reflex. The specificities for the MTI photoscreener versus the Brückner reflex were similar at 69% and 71%, respectively. They concluded that Pediatric residents were better at detecting asymmetric red reflexes in patients with anisometropia and microstrabismus when evaluating MTI photoscreener photographs than when evaluating the red reflexes by the Brückner reflex. The MTI photoscreener may be a more sensitive method than the Brückner reflex to screen for the common amblyogenic risk factors of anisometropia and microstrabismus by easier detection of red reflex asymmetry. The findings of this study were similar to the findings of our study that automated photoscreening using photoscreeners is a more sensitive and specific as compared to manually performed red reflex testing.
Limitations in our study
- A major limitation is difficulty in quantifying the results. This difficulty may also cause inter-observer and intra-observer variations.
- We found that lack of accommodative control and absence of distance fixation target can cause pseudomyopia that can reduce the specificity and predictive value of the positive test.
- The test is rendered useless with dilated pupil.
- Though we did not have a patient with high ametropia we are aware that patients with high myopia have a dark fundal glow and patients with high hypermetropia have a bright fundal glow. In both the situations there is an absence of the crescent. The examiner should be aware of this situation and diagnose these patients as having high ametropia.
- Variability in the pigmentation of the fundus has previously been reported to affect the sensitivity of the Brückner test when used to detect amblyogenic factors—darker fundus pigmentation is associated with lower sensitivity. It is not clear what effect pigmentation of the fundus may have on the Brückner test when used to detect refractive errors.
- As the Brückner test provides possibilities to introduce lower cutoffs for the crescent size that may improve sensitivity and negative predictive value at the cost of increasing the false positives. We are concerned about the relatively higher false positive cases value obtained for the red reflex testing done by Pediatric resident in our study. The issue of false positives is of importance, as these subjects are referred to Ophthalmologist for more sophisticated and often more expensive tests, placing an additional burden on healthcare programs. This limitation can be overcome with more training and the examiners must decide cutoffs to provide maximum effectiveness to the screening program.
Conclusions: Our study on screening of eye diseases using red reflex testing by a Pediatric resident concludes that the photoscreener has a higher specificity and sensitivity in detecting refractive errors and astigmatism as compared to manually performed red reflex testing. But in absence of costly ophthalmic instruments like the photoscreener, red reflex testing is a good screening test in routine Pediatric OPD as it is low cost, less time consuming ,can be done with a direct Ophthalmoscope only, is fairly sensitive and has a high negative predictive value .
We conclude that red reflex testing – 1) Is a relatively easy and simple test to administer, 2) Can train persons with no or minimal prior experience 3) Can be administered using only a direct Ophthalmoscope, thereby minimizing costs when compared to a photoscreener 4) Can potentially screen a large population within a short period as the test does not take long to administer 5) The test has good sensitivity 6) With experience the sensitivity and specificity improves 7) The investigator can proceed with the additional examination using the same Ophthalmoscope 8) It is a useful test in screening of children for eye diseases in routine Pediatric practice .
Leave a Comment