
 FP1238 : Comparison between Image guided system and Smartphone marker app for toric IOL cataract surgery
FP1238 : Comparison between Image guided system and Smartphone marker app for toric IOL cataract surgeryDr. SWATI AGARWAL
Dr.Ajoy Paul, Dr.Sagar Bhargava
Semi Finals
Abstract
The pupose of this study is to compare the clinical outcomes between Verion Image-Guided System versus a Smartphone digital reference marker app for toric intraocular lens (IOL) implantation in cataract surgery. Study was conducted in tertiary eyecare centre, India. Eyes with regular corneal astigmatism of more than 1.5 dioptres (D) that required cataract surgery and toric IOL implantation (Acrysof SN6AT3-T9) were randomly assigned to the image-guided group or the smartphone app digital reference marker group. Postoperative outcome was measured by uncorrected distance visual acuity (UCDVA), residual astigmatism and deviation from the target anticipated residual astigmatism. Results demonstrated that using VERION image guided digital marking system over smartphone digital reference marking app did not lead to significant improvement with respect to clinical outcomes.
Full Text
Purpose: To compare the clinical outcomes between Verion Image-Guided System versus a Smartphone digital reference marker app for toric intraocular lens (IOL) implantation in cataract surgery.
Setting: Tertiary Eyecare Centre, India
Design: Prospective randomized clinical study.
Methods: Eyes with regular corneal astigmatism of more than 1.5 dioptres (D) that required cataract surgery and toric IOL implantation (Acrysof SN6AT3-T9) were randomly assigned to the image-guided group or the smartphone app digital reference marker group. Postoperative outcome was measured by uncorrected distance visual acuity (UCDVA), residual astigmatism and deviation from the target anticipated residual astigmatism.
Results: The study enrolled 23 eyes (20 patients). The postoperative UCDVA of all the eyes in both the groups were Snellens 6/9; LogMAR 0.18 and better. The mean postoperative UCDVA for the image marking group was 0.14 ± 0.066 logarithm of minimum angle of resolution (LogMAR) and for the smartphone toric marking app group was 0.138 ± 0.058 LogMAR (t test 0.942). The mean residual refractive cylinder was 0.154 ± 0.184 D and 0.175 ± 0.195 D in the image-guided group and smartphone toric marking app group, respectively (t test 0.804). The mean of the deviation between target anticipated residual astigmatism and actual residual astigmatism in the image guided group was 0.197 ± 0.158 D versus 0.157 ± 0.129 D in the smartphone toric marking app group (t test 0.532).
Conclusion: There was no significant difference in UCDVA, residual refractive astigmatism or deviation from target anticipated residual astigmatism between the image guided digital marking system versus smartphone digital reference marker app in Toric IOL cataract surgery.
It has been estimated that 30% of patients with cataract have more than 0.75 D of corneal astigmatism, that 22% have more than 1.50 D, and that 8% have more than 2.00 D of corneal astigmatism [1,2]. Toric IOLs are an indispensable tool for optimising refractive outcomes, visual performance and patient satisfaction after cataract surgery [3,4]. Toric IOLs provide better postoperative UCDVA, greater spectacle independence, and lower postoperative astigmatism compared to non-toric and non-toric IOLs + relaxing incision [5].
Today’s cataract patients expect optimal vision after intraocular lens implantation, and those who choose toric IOLs do not expect to have to wear glasses or contact lenses full time after cataract surgery. The accuracy of the toric IOL surgery depends on the following factors: Appropriate patient selection, accuracy of the biometry and keratometry, accuracy of the calculator being used, accuracy of the preoperative reference markings [6,7], accuracy of the IOL placement in the capsular bag and rotational stability of the IOL
Prediction of astigmatic outcomes with toric IOLs can be improved with appropriate measuring devices and methods to establish the required toric IOL power. Keratometric readings can be obtained by different devices like automatic and manual keratometry, Topographer, Verion, etc. In case of discrepancy between values an integrated K reading can be generated using vector analysis in the current Barrett’s toric calculator. The integrated K is significantly more accurate than a value from a single device and thus significantly eliminates any keratometric errors [8]. The Barrett toric calculator had the lowest mean absolute error in predicted residual astigmatism (0.35 to 0.54 D, all devices) compared with the Alcon and Holladay toric calculators with or without the Baylor nomogram (P <.021) [9]. The new Barrett calculator theoretically accounts for Posterior corneal astigmatism (PCA) [10] in With the rule (WTR) and Against the rule (ATR) astigmatic eyes [9], axial length and anterior chamber depth in Effective lens position (ELP) estimates permitting more precise astigmatic prediction [11]. Barrett online toric calculator is thus the most accurate online toric calculator available as of date [10].
IOL alignment is crucial to refractive success; for every degree of misalignment, there is a reduction of 3.3% of the astigmatism correction [12]. The manual preoperative reference markings are done with patient sitting and head erect. These markings can be slit-lamp assisted with pendulum or gravity marker, bubble marker, free hand, or with smartphone digital reference marker app [13-15].
Smartphone assisted digital reference marking is a simple, inexpensive, and precise method to measure the toric IOL axis using a camera-enabled and gyroscope assisted cellular phone [16]. Applications like the “iToric Patwardhan” on the android platform (Dr S. Patwardhan) and the ‘toriCAM’ [17] on the iOS platform (Dr G. Barrett – iOS), are available free of cost and can determine the exact axis of the corneal limbal marks as a reference to find the correct alignment for a toric IOL during surgery. Alternatively natural landmarks of the conjunctiva can be used instead of applying ink marks on the limbus to get a digital reference.
Mark-less IOL alignment can be achieved by image-guided systems like VERION image-guided system (Alcon, Fort Worth, Texas), CALLISTO Eye and Z align (Carl Zeiss Meditec, Jena, Germany), and TrueVision 3D Surgical system, Santa Barbara, California). Image guided systems also aid in planning the incisions, capsulorhexis size, and optimal IOL centration. VERION Digital Marker (VDM) uses multiple reference points on the conjunctiva and limbus such as scleral vessels, limbal vessels and iris features to create a digital overlay between the live surgery image and image taken preoperatively. It then projects the desired implantation axis of the toric IOL into the right ocular of the surgeon’s microscope while using eye tracking navigation to account for cyclotorsion and eye movement. Thus, VERION Image guided system claims to ‘minimise data transcription errors, improvement in clinical efficiency, toric and multifocal IOL confidence, ensures surgical consistency, and optimises visual outcomes’ [18].
VERION™ guidance delivers better outcomes than slit-lamp assisted and conventional manual ink-marking techniques in terms of induced astigmatism [19-22]
In this study, we intend to compare between the VERION image-guided system and the iToric Smartphone digital reference marker app, clinical outcomes with respect to uncorrected distance visual acuity (UCDVA), residual astigmatism and deviation from target residual astigmatism in a toric IOL cataract surgery. To our knowledge there has been no previous published studies or reports of this.
METHOD
This is a prospective randomised clinical study conducted at a tertiary eyecare centre. The study included 23 eyes of 20 patients undergoing phacoemulsification cataract surgery with coexisting corneal astigmatism more than 1.5 dioptre (D). The eyes were randomly assigned to either digital image guidance using VERION digital marker or Smartphone app assisted digital reference marking. Sample size for smartphone digital reference marking app group was 10 (n=10) and for the VERION image guided digital marking system group was 13 (n=13).
Detailed slit-lamp evaluation was done for every patient and those with corneal or retinal pathologies, irregular astigmatism, high axial length, history of previous ocular or intraocular surgery, ocular trauma and amblyopia were not included in the study.
A compromised ocular surface may skew keratometric measurements by up to 2.5D [23]. Topography has been done for every patient to evaluate and rule out patients with irregularities on the ocular surface. Irregular topography can indicate corneal disease, such as severe dry-eye disease, ocular surface disease, basement membrane dystrophy or some other subtle corneal pathology that may have been missed. Diffuse irregularity on topography is often consistent with dry-eye disease, and this can be confirmed using vital dye staining and examining tear breakup time at the slit lamp. One of these conditions could be inducing the astigmatism.
OCT was preoperatively done for every patient to rule out any apparent or obvious retinal pathology.
Keratometry was performed on multiple devices viz auto and manual keratometer, topographer for smartphone assisted making group. Keratometric analysis on VERION was done in addition for the VERION image guided IOL implantation group. Integrated K reading was taken in calculation whenever there was a discrepancy in K readings between the devices. Biometry was performed by Immersion method in all the cases. Toric IOL power and axis of implantation was decided by Barrett online toric calculator.
For the smartphone app digital reference marker group, with the patient seated on operation table, an arbitrary point was marked at the limbus. The point was sharp and did not smudge. A flashlight was shone at glabella and patient focussed straight on a distant point. Using the gyroscope assisted camera of iToric app a snap was taken. Image was zoomed to fit the outer circle at limbus. Using the protractor, the red line was dragged to pass through the centre of cornea and the red dots were placed on the marks at limbus to get the axis of marks [Fig.1]. By taking into account the gyroscopic assisted camera rotation, we get the effective mark rotation from the 0-180 axis. Thereafter on operation table after sterile draping, Mendez ring was aligned at 0-180 degree by keeping the mark at effective rotation axis.
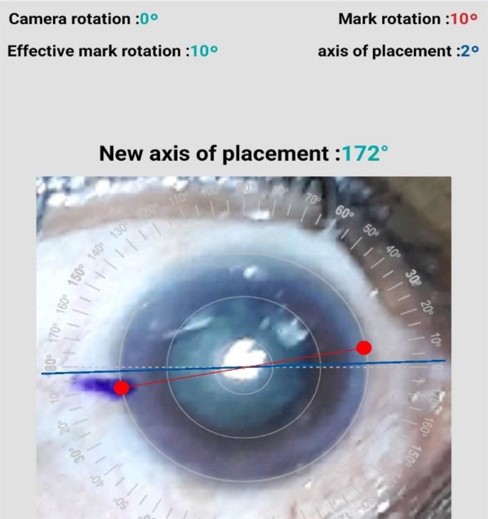


Figure1: Finding the exact axis of marks with the iToric app by dragging the red line through centre of cornea and on the marks.
For the VERION Image guided group, after planning of the surgical procedure in VERION reference unit, data was exported to VERION digital marker (VDM) located in the operating room. This allows the surgeon to see in one of the oculars of the operating microscope in real-time a digital tracking overlay picture after the intraoperative image registration. This system automatically corrects the cyclotorsion by recognising scleral vessels and landmarks of the iris and visually guides the surgeon for the size and location of corneal incisions and capsulorhexis [fig 2] It shows the axis of IOL implantation and also assists the surgeon in controlling the IOL centration.

Figure 2: VERION overlay showing the location of corneal incisions
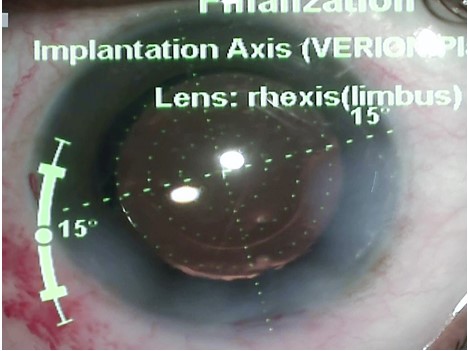
Figure 3: VERION overlay showing the implantation axis
To reduce any IOL related confounding factors like rotational stability, Acrysof IQ Toric platform (SN6AT3-T9) was used in all cases [24]. Surgeries were performed by a single surgeon to reduce any surgeon related variables like surgically induced astigmatism (SIA), effective lens position (ELP), IOL alignment techniques, etc. Surgeries were done with 2.8 mm main incision at 90 degrees. No intraoperative complication was encountered in any of the cases. In postoperative period, IOL alignment was checked on slit lamp at 1 hour. At postoperative 14 days, patient was evaluated for IOL rotation. However, no rotation was encountered in our study.
Residual astigmatism decreases the postoperative visual outcome with respect to optical clarity, contrast sensitivity and overall patient satisfaction [25]. In this study we use UCDVA, BCDVA, Residual astigmatism, deviation from target residual astigmatism as a measure of the clinical outcome of toric IOL surgery.
Data was entered in Microsoft Excel. Using the software, mean and standard deviation was calculated for the different samples and unequal Variance (Independent) unpaired t-test was done to analyse for any significant difference between the two groups.
Results
23 eyes of 20 patients were used for data analysis of which the sample size smartphone digital reference marking app group was 10 and for the VERION image guided digital marking system group was 13. Unequal variance unpaired t test was used to analyse. Results of the analysis are shown in table1. The postoperative UCDVA of all the eyes in both the groups were Snellens 6/9; LogMAR 0.18 and better.
The mean postoperative UCDVA for the image marking group was 0.14 ± 0.066 logarithm of minimum angle of resolution (LogMAR) and for the smartphone toric marking app group was 0.138 ± 0.058 LogMAR (t test 0.942).
The mean postoperative BCDVA for the image guided digital marking group was 0.10 ± 0.065 LogMAR and for the smartphone digital reference marking app group was 0.074 ± 0.079 LogMAR (t test 0.407).
The mean residual refractive cylinder was 0.154 ± 0.184 D and 0.175 ± 0.195 D in the image-guided group and smartphone toric marking app group, respectively (t test 0.804)
The mean of the deviation between target anticipated residual astigmatism and actual residual astigmatism in the image guided group was 0.197 ± 0.158 D versus 0.157 ± 0.129 D in the smartphone toric marking app group (t test 0.532)
| Smartphone digital reference marking app group | VERION image guided digital marking group | t test | |
| UCDVA | 0.138 ± 0.058 LogMAR | 0.14 ± 0.066 LogMAR | 0.942 |
| BCDVA | 0.074 ± 0.079 LogMAR | 0.10 ± 0.065 LogMAR | 0.407 |
| Residual astigmatism | 0.175 ± 0.195 D | 0.154 ± 0.184 D | 0.804 |
| Deviation of residual astigmatism from target anticipated astigmatism | 0.157 ± 0.129 D | 0.197 ± 0.158 D | 0.052 |
Table1: Comparison between Smartphone digital reference marking and VERION image guided digital marking
DISCUSSION
Our results demonstrated that there is no significant difference between the uncorrected refractive error, residual astigmatism, or deviation from target residual astigmatism in both the image guided digital marking group and the smartphone digital reference marker app group.
This demonstrates that using VERION image guided digital marking system over smartphone digital reference marking app did not lead to significant improvement with respect to clinical outcomes.
It should be noted that there are some important differences between the present study and the previously conducted studies. The earlier studies demonstrated a strong agreement between the between the VERION and smartphone axis marking but assumed VERION image guided system as the gold standard for accurate alignment of the toric IOLs [26]. A considerable advantage in the design of the current study is the ability to independently evaluate and compare the clinical outcomes of the two marking systems.
Smartphone digital reference marker apps are a cheap consistent and reproducible way of enhancing outcomes of Toric IOLs. Ophthalmic toric marking apps are easily available and can turn smartphones into sophisticated medical devices. It should be noted that smartphone assisted digital reference marking needs a lot of care, precision and is prone to transcription errors.
VERION image guided system aims to make the process of toric IOL alignment more accurate and potentially offers a way to limit sources of error. It enhances the surgical flow especially in a high-volume centre and reduces the surgical time. Sometimes intraoperative registration may not be successful if the patient is uncooperative or anxious or there is a development of conjunctival chemosis. Also due to its high cost, it may not be an economically viable option for majority of ophthalmologists. There is no doubt that the estimation of the ability of any device to provide repeatable, reproducible and reliable outcomes is equally significant as the evaluation of its other characteristics. The measurements performed with the SensoMotoric instrument (SMI) Reference Unit showed an acceptable intrasession repeatability for astigmatism magnitude, but a moderate repeatability for the meridians of astigmatism [27]. So, an evaluation of intra-observer and inter-observer variability of VERION reference system should be done in future.
The limitation of this study is that it provides results obtained by a single surgeon. Though this helps eliminate surgeon variables like surgically induced astigmatism, ELP, surgeon related alignment accuracy; a multivariate evaluation should be performed in the future to evaluate the clinical accuracy of the two systems in different hands.
Conclusion
There was no significant difference in UCDVA, residual refractive astigmatism or deviation from target anticipated residual astigmatism between the image guided digital marking system versus smartphone digital reference marker app in Toric IOL cataract surgery.
Acknowledgements
The ‘iToric Patwardhan‘ mentioned in the study is a free app available on android smartphones and developed by Dr Sourabh Dileep Patwardhan. The authors have no financial or propriety interests in it.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
References
- B. V. Ventura, L. Wang, M. P. Weikert et al., “Surgical management of astigmatism with toric intraocular lenses,” Arquivos Brasileiros de Oftalmologia, vol. 77, no. 2, pp. 125–131, 2014.
- AC Day et al., “Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK”, Br J Ophthalmol, doi: 10.1136/ bjophthalmol-2018-312025. PMID:30190365.
- N Visser et al., “Toric vs aspherical control intraocular lenses in patients with cataract and corneal astigmatism: a randomized clinical trial”, JAMA Ophthalmol, 132, 1462-1468 (2014). PMID: 25256624.
- D Mingo-Botin et al., “Comparison of toric intraocular lenses and peripheral corneal relaxing incisions to treat astigmatism during cataract surgery”, J Cataract Refract Surg, 36, 1700-1708 (2010). PMID: 20870116.
- L Kessel et al., “Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis”, Ophthalmol, 123, 275-286 (2016). PMID: 26601819
- Visser N, Berendschot TT, Bauer NJ, Jurich J, Kersting O, Nuijts RM. Accuracy of toric intraocular lens implantation in cataract and refractive surgery. J Cataract Refract Surg. 2011;37(8):1394‐1402. doi:10.1016/j.jcrs.2011.02.024
- Farooqui JH, Sharma M, Koul A, Dutta R, Shroff NM. Evaluation of a new electronic preoperative reference marker for toric intraocular lens implantation by two different methods of analysis: Adobe Photoshop versus iTrace. Oman J Ophthalmol. 2017;10(2):96‐99. doi:10.4103/ojo.OJO_163_2013
- eurotimes.org/eliminating-astigmatic-defocus/#.XsfzVX6pxiA
- A Abulafia et al., “Prediction of refractive outcomes with toric intraocular lens implantation”, J Cataract Refract Surg, 41, 936-944 (2015). PMID: 25936681.
- Koch DD, Ali SF, Weikert MP, Shirayama M, et al. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg 2012;38:2080-2087
- Barrett GD, Innovative toric IOL calculators and how to use them: Barrett Toric Calculator. Cataract & Refract Surg Today Europe. May 2015 supplement].
- Felipe A, Artigas JM, Diez-Ajenjo A, Garcia-Domene C, Alcocer P. Residual astigmatism produced by toric intraocular lens rotation. J Cataract Refract Surg 2011;37(10):1895-1901.
- Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631‐1636. doi:10.1016/j.jcrs.2008.04.041
- Carey PJ, Leccisotti A, McGilligan VE, Goodall EA, Moore CB. Assessment of toric intraocular lens alignment by a refractive power/corneal analyzer system and slitlamp observation. J Cataract Refract Surg. 2010;36(2):222‐229. doi:10.1016/j.jcrs.2009.08.033
- Cha D, Kang SY, Kim SH, Song JS, Kim HM. New axis-marking method for a toric intraocular lens: mapping method. J Refract Surg. 2011;27(5):375‐379. doi:10.3928/1081597X-20101005-01
- Teichman JC, Baig K, Ahmed II. Simple technique to measure toric intraocular lens alignment and stability using a smartphone. J Cataract Refract Surg. 2014;40(12):1949‐1952. doi:10.1016/j.jcrs.2014.09.029
- Pallas A, Yeo TK, Trevenen M, Barrett G. Evaluation of the Accuracy of Two Marking Methods and the Novel toriCAM Application for Toric Intraocular Lens Alignment. J Refract Surg. 2018;34(3):150‐155. doi:10.3928/1081597X-20180115-03
- www.myalcon.com/products/surgical/verion-guided-system
- AH Elhofi and HA Helaly, “Comparison between digital and manual marking for toric intraocular lenses: a randomized trial”, Medicine, 94, e1618. PMID: 26402830]
- Panagiotopoulou, Eirini-Kanella et al. “Image-guided lens extraction surgery: a systematic review.” International journal of ophthalmologyvol. 12,1 135-151. 18 Jan. 2019, doi:10.18240/ijo.2019.01.21
- Mayer WJ, Kreutzer T, Dirisamer M, et al. Comparison of visual outcomes, alignment accuracy, and surgical time between 2 methods of corneal marking for toric intraocular lens implantation. J Cataract Refract Surg. 2017;43(10):1281‐1286. doi:10.1016/j.jcrs.2017.07.030
- Webers VSC, Bauer NJC, Visser N, Berendschot TT, van den Biggelaar FJ, Nuijts RMMA. Image-guided system versus manual marking for toric intraocular lens alignment in cataract surgery. J Cataract Refract Surg 2017;43;781-8.
- AT Epitropoulos et al., “Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning”, J Cataract Refract Surg, 41, 1672-7 (2015). PMID: 26432124
- BS Lee and DF Chang, “Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes”, Ophthalmology, 125, 1325-1331 (2018). PMID: 29544960.
- Titiyal JS, Kaur M, Jose CP, Falera R, Kinkar A, Bageshwar LM. Comparative evaluation of toric intraocular lens alignment and visual quality with image-guided surgery and conventional three-step manual marking. Clin Ophthalmol. 2018;12:747‐753. Published 2018 Apr24.doi:10.2147/OPTH.S164175
- Khatib ZI, Haldipurkar SS, Shetty V. Verion digital marking versus smartphone-assisted manual marking and isolated manual marking in toric intraocular lens implantation. Indian J Ophthalmol. 2020;68(3):455‐458. doi:10.4103/ijo.IJO_987_19
- Visser N, Berendschot TT, Verbakel F, de Brabander J, Nuijts RM.Comparability and repeatability of corneal astigmatism measurements using different measurement technologies. J Cataract Refract Surg 2012;38(10):1764-1770.
Leave a Comment